The Pathfinder™ ACL System consists of a reusable surgical instrument – the Pathfinder ACL Guide – and a flexible Pathfinder Guide Pin with sheath. Together, they provide the surgeon with a unique ability to achieve anatomic femoral tunnel placement with minimal complexity. The system can accommodate any tibial tunnel aperture or orientation, is equally facile with soft tissue or BTB grafts, and is compatible with all commercially available reamers.
Hybrid Transtibial Technique (HTT) vs. Transtibial Technique (TT)
The HTT represents a minor modification of the conventional Transtibial Technique (TT). As with TT, the femoral guide wire is inserted through the tibial tunnel to drill the femoral tunnel.
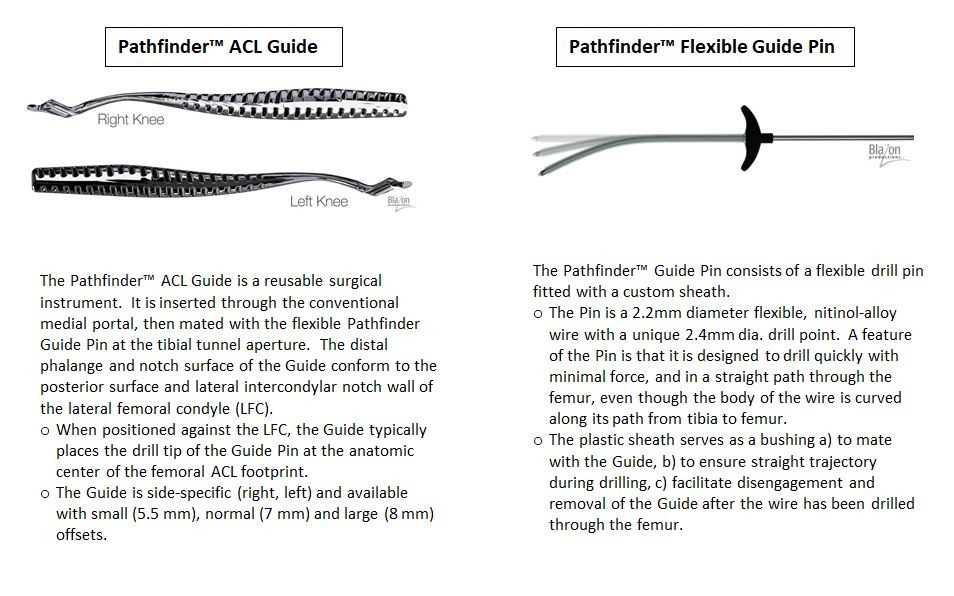
The primary difference with HTT involves both the Pathfinder ACL Guide, the flexible nature of the Pathfinder Guide Pin and the sheath on the Guide Pin. The Guide is capable of directing the transtibial guide wire* without being constrained by the tibial tunnel. This is achieved via the instrument’s open-slot configuration which allows it to capture and direct the flexible transtibial wire to the femoral insertion from the medial portal. The sheath on the Guide Pin acts as a bushing to mate closely with the Guide and to control drilling. [* the terms "guide wire" and "guide pin" are used interchangeably.]
The absence of tibial tunnel constraint with this approach allows the transtibial guide wire to be consistently positioned in an anatomic position on the lateral wall, something a conventional TT cannot consistently accomplish. Because HTT maintains a transtibial path for drilling and reaming, however, the beneficial aspects of TT are still preserved:
- Eliminates the weaknesses of TT:
- The HTT enables anatomic femoral tunnel positioning
- Accommodates any tibial tunnel, thus eliminating the need for careful tibial tunnel orientation
- Maintains the strengths of TT:
- Knee can remain at 90 degrees of flexion
- Femoral aperture shape is highly anatomic
- Femoral tunnel length is maintained, minimizing the risk of graft tunnel mismatch
- No posterior wall blowout
- Minimal tunnel angulation, allowing easy graft passage and preventing killer turn
Hybrid Transtibial Technique (HTT) vs. Anteromedial Portal Technique (AM)
The HTT is a major simplification of the AM Portal Technique.
While both methods can place the femoral guide wire at the center of the native ACL footprint, the AM Portal approach requires drilling and reaming to be performed through the medial portal. This requirement increases technical difficulty as it requires hyperflexion of the knee – limiting visualization and requiring an extra shuttling step for graft passage – and puts the articular cartilage at risk of injury as the reamer passes in front of the medial femoral condyle.
Further, because the reamer approaches the lateral wall less obliquely with AM, tunnel apertures are more circular than the native femoral insertion.
Finally, AM portal femoral tunnels tend to be much shorter, more angulated and with a greater risk of posterior wall blowout.
Because the HTT allows drilling and reaming to stay along a transtibial path, these drawbacks are avoided:
- Eliminates the weaknesses of AM portal:
- No need to hyperflex the knee, improving notch visualization and overall technical ease
- No risk of articular cartilage injury because reamer remains transtibial
- Anatomic orientation of reamer to lateral wall produces anatomic aperture shape
- Femoral tunnel lengths are maintained, avoiding graft tunnel mismatch
- No posterior wall blowout
- Minimal femoral tunnel angulation, allowing easy graft passage and preventing killer turn
- Prevents extra suture shuttling step during graft passage
- Maintains the strengths of AM Portal:
- The HTT enables femoral aperture positioning equally as anatomic as AM Portal.
- The HTT enables femoral aperture positioning equally as anatomic as AM Portal.
Overview of the Pathfinder HTT procedure
|
(1) As in the conventional Transtibial Technique procedure, the tibial tunnel is drilled first with a rigid guide pin, then reamed with a standard cannulated reamer. |

|
(2) The Pathfinder ACL Guide is inserted through the medial portal and positioned with the slot entrance above the tibial opening. |
|
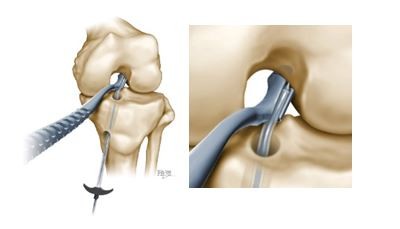
(3) The flexible Pathfinder Guide Pin is inserted through the tibial tunnel and fully engaged within the slot of the Pathfinder Guide. |
|
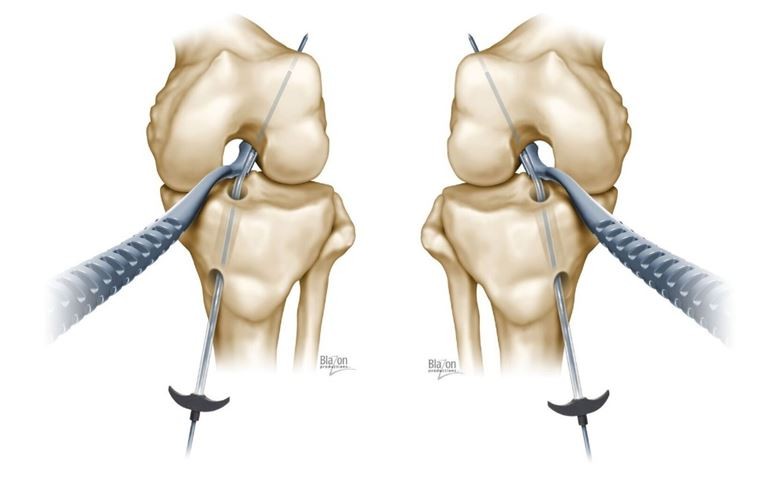
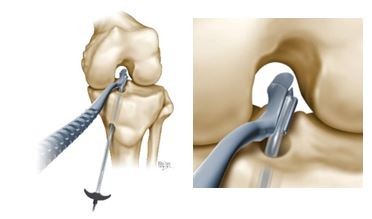
(4) The Pathfinder Guide/Guide Pin assembly is advanced through the lateral intercondylar notch. The curved distal phalange is then positioned behind and firmly against the posterior condyle surface. The notch surface of the Guide is then firmly seated against the notch wall of the condyle. At that point, the drill tip of the wire should automatically be positioned accurately at the center of the femoral ACL footprint. The point of intersection can easily be adjusted, if desired. |

|
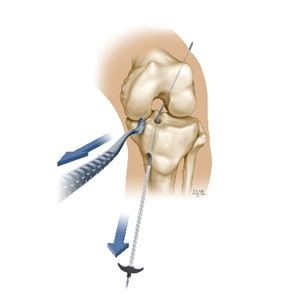
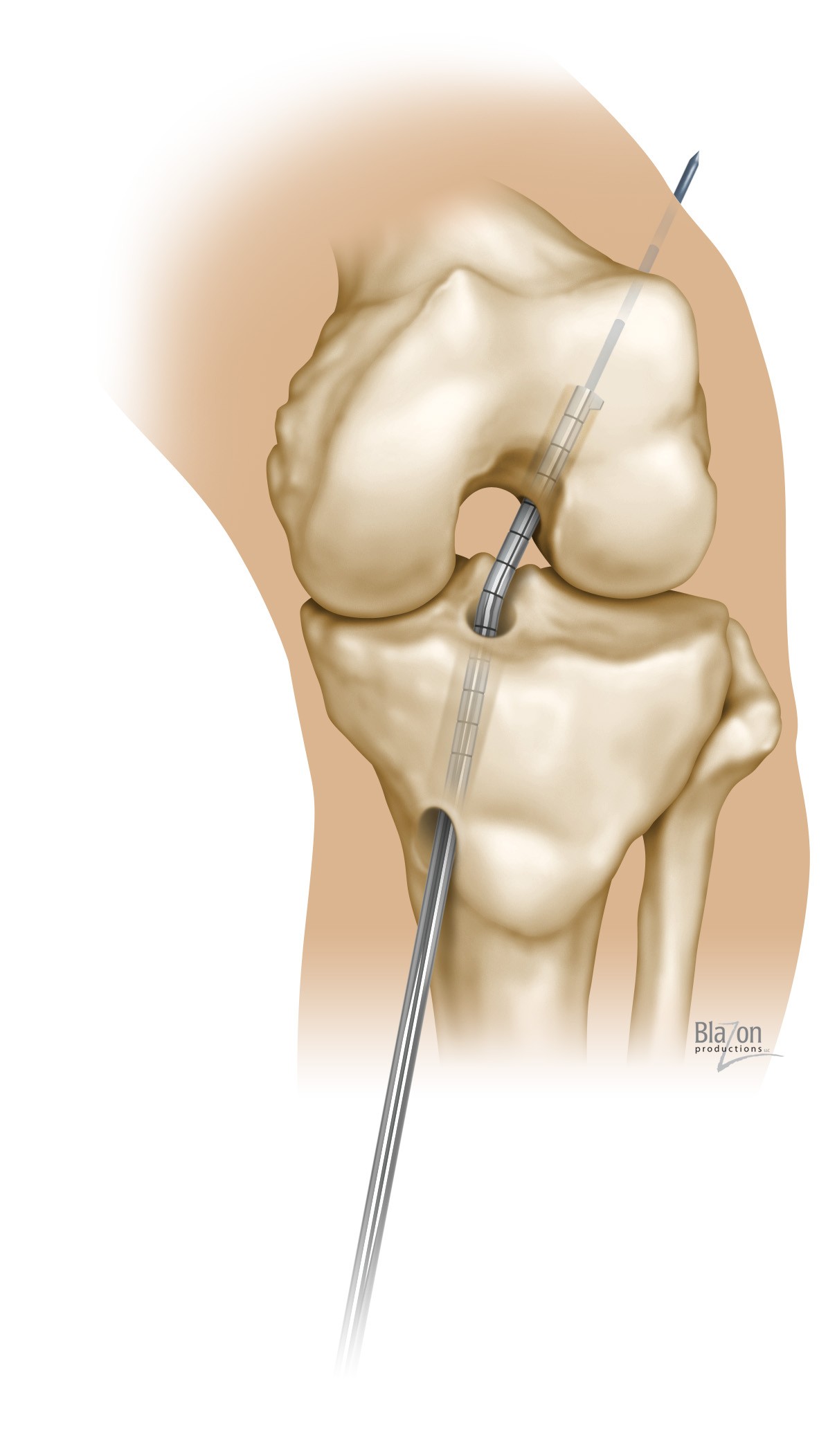
(5) Once the wire is positioned appropriately, it is drilled through the femur. It will exit the distal thigh above the mid-line. |
|
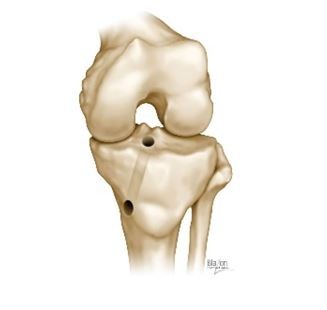
(6) The sheath is pulled proximally off the Guide Pin, enabling the Pathfinder Guide to be extricated from the Guide Wire and removed from the knee joint. The result is an anatomically positioned transtibial guide wire. |
|
(7) The femoral tunnel is then reamed via the tibial tunnel using a flexible reamer. [Alternatively – if a flexible reamer is not available – a rigid reamer may be used from outside-in (antegrade) over the exiting guide wire at the distal thigh.]
|
Throughout the procedure the knee remains at 90⁰.
Click on the links below for more information: