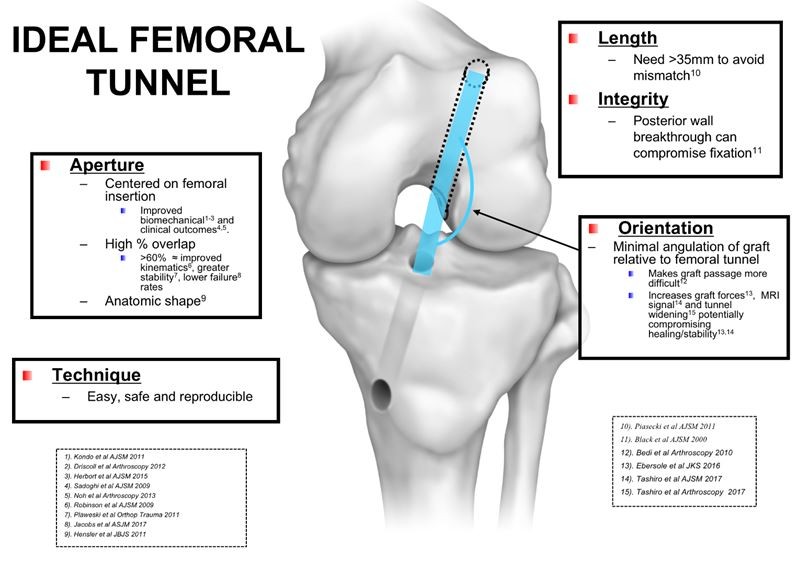
The ideal femoral tunnel optimizes a number of different features:
- Anatomic aperture position: The literature* supports improved biomechanical, kinematic and clinical outcomes when the femoral aperture is positioned in the center of the native ACL femoral footprint.
[*See References and Resources Section] - Adequate length: Long femoral tunnels (>35 mm in the average patient) minimize the risk of significant graft-tunnel mismatch.
- Intact posterior wall: Avoiding posterior wall breakthrough is important for ensuring secure femoral tunnel graft fixation.
- Minimally angulated: Tunnels that are significantly angulated from the straight-line intraarticular path of the graft will make graft passage more difficult and increase strain on the graft at the femoral tunnel aperture.
- Easy, Safe and Reproducible Technique: Whatever technique is utilized for femoral tunnel preparation should be technically consistent, easy and with a low risk of complication.
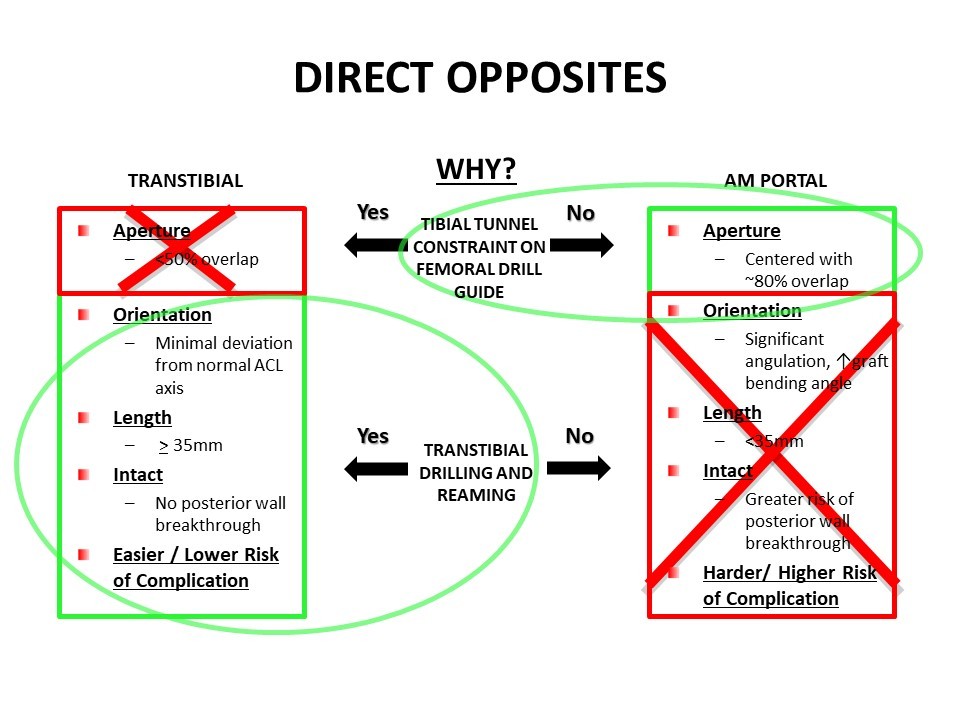
The most common femoral tunnel positioning techniques currently used – Transtibial and AM Portal approaches – have opposing strengths and weaknesses relative to these ideal characteristics.
Transtibial Technique
The traditional Transtibial Technique is safe, easy and reproducible, has a low risk of complication and consistently produces long, intact and minimally angulated tunnels. Because a Transtibial technique imposes constraint on the femoral drill guide along its transtibial path, however, the primary limitation of this approach is its inability to consistently achieve anatomic femoral tunnel aperture positions.
A number of studies* have demonstrated that the best a Transtibial Technique can consistently achieve in aperture positioning – assuming an anatomic tibial tunnel aperture and a structurally intact tibial tunnel – is roughly 50% overlap with the native femoral insertion. [*See References and Resources Section]
![]()
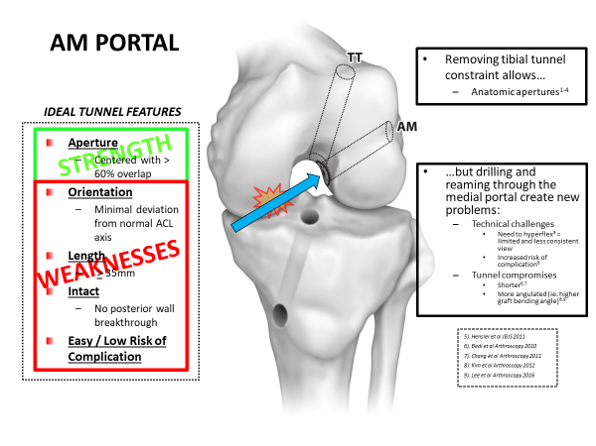
AM Portal Technique
By contrast, an AM Portal Technique eliminates tibial tunnel constraint – by inserting the drill guide through the medial portal instead of the tibial tunnel - and has been shown* to achieve consistent anatomic femoral tunnel aperture positioning. [*See References and Resources Section]
However, while solving the “aperture problem” of a Transtibial Technique, this approach is limited by its need to also drill and ream through the medial portal, a technical characteristic that eliminates all the other benefits of Transtibial Technique. Specifically...
- Drilling and reaming through the medial portal increases technical difficulty by requiring the knee to be hyperflexed, which creates a more variable and limited visualization of the intercondylar notch.
- Passage of the reamer in front of the medial femoral condyle also risks damage to the articular surface.
- Additionally, the more horizontal trajectory of the wire and reamer relative to the lateral wall of the notch will produce more circular (less anatomic) aperture shapes, and femoral tunnels that are much shorter, more angulated and with a greater propensity for posterior wall breakthrough.
Transtibial vs. AM Portal Techniques
When these technique characteristics are compared, it is noteworthy that Transtibial and AM Portal techniques are direct opposites, each sacrificing the strengths of the other. An ideal technique might aspire to combine the beneficial technical features of these two common approaches.
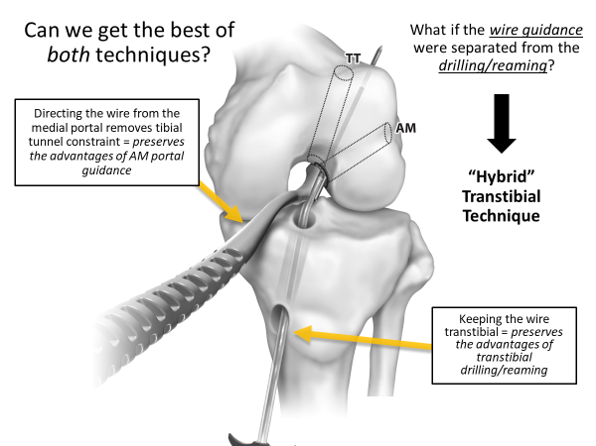
The Solution: Combine the advantages of both Transtibial and AM portal techniques
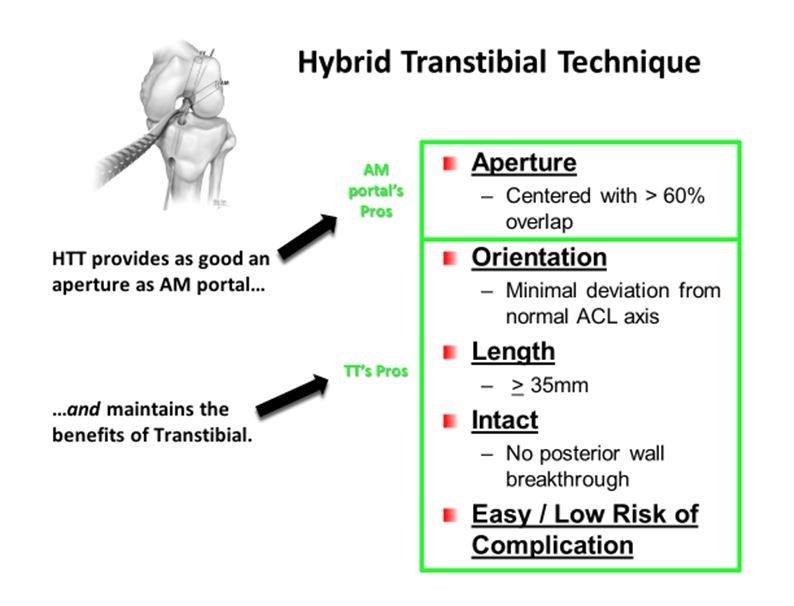
A hybrid of the Transtibial and AM portal techniques combines the best of both techniques. The Hybrid Transtibial Technique (HTT) simultaneously directs the femoral guide wire independent of the tibial tunnel, but also maintains a transtibial path for the wire and reamer.
This is accomplished with the novel Pathfinder Guide and Guide Pin. Together, these devices allow separate portals of entry for the femoral drill guide and the guide wire. The Guide has the capacity to capture – and then anatomically direct – the transtibial wire inside the joint. This feature allows the femoral tunnel location and direction to be independent of the direction of the transtibial guide wire, combining the best of both Transtibial and AM Portal approaches:
The benefits of the Hybrid Transtibial Technique therefore include the combination of anatomic femoral tunnel apertures with long, minimally angulated and intact femoral tunnels and an easy, reproducible and safe approach. A recently published cadaveric study (Jennings et al OJSM 2017)* comparing all three techniques demonstrated these beneficial characteristics. (*See References and Resources Section)
As a result of these advantages, the HTT has a wider application to ACL reconstruction than other available techniques. In addition to providing a consistent technique for every primary ACL, this approach provides advantages for:
- Pediatric ACL reconstruction:Transtibial-like tunnel angulation means less overlap with the femoral physis than an AM portal technique.
- Revision ACL reconstructions. When revising a failed prior Transtibial reconstruction, the HTT offers the ability to revise the femoral tunnel using the same tibial tunnel. (Click to see example of an HTT revision surgery)
Summary
By combining the strengths – and eliminating the weaknesses – of the two most common ACL reconstruction techniques, the HTT represents a positive evolution in ACL femoral tunnel positioning. From a practical standpoint, this technique offers the surgeon an easier, better way to manage ACL deficiency across a wider spectrum of clinical scenarios.
Click on the links below for more information: